Converting cascade impaction data into the aerodynamic particle size distribution (APSD) metrics that define orally inhaled product (OIP) performance.
Your optimal cascade impactor test set-up is working well, assays complete and analyses successfully run. What next? In its raw form cascade impaction data is less than optimal for assessing the likely success of drug delivery, or batch-to-batch equivalence. Processing it to generate meaningful metrics that capture the complexities of APSD is the way forward.
In this blog we’re examining the path from cascade impaction data to critical quality attributes, for OIPs. The key metrics of mass median aerodynamic diameter (MMAD), geometric standard deviation (GSD) and fine particle fraction (FPF) are the primary focus. But we’re also considering the principles and output of efficient data analysis (EDA). Our focus is not the maths – there is software for that – but rather the concepts, the metrics that we use to characterise OIPs and why.
Understanding the raw data
A first point to note is that a cascade impactor does not size the entire emitted dose from an OIP. Rather it characterises the impactor sized mass (ISM), the fraction of most interest for pulmonary drug delivery. Non-sizing elements of the test set-up include the mouthpiece, the induction port and potentially the preseparator (depending on the selected impactor). Measuring drug deposition data for these elements is useful but provides little insight into particle size.
Focusing on ISM, we know that impactor performance is flow rate dependent. Raw cascade impaction data therefore takes the form of drug substance mass per stage, with flow rate defining stage cut-off diameter. Examples of such data are shown below in the form of cumulative (left) and log-probit (right) plots.
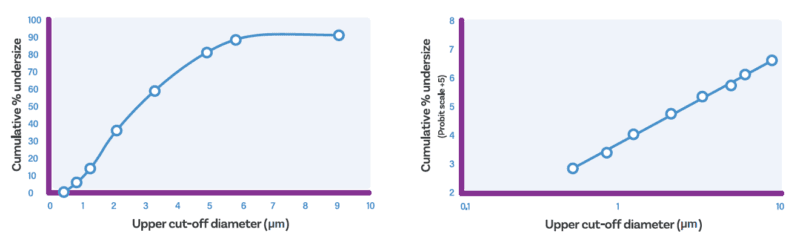
A simple cumulative undersize curve (left) and a log-probit plot (right)
Defining and determining MMAD
MMAD is one such metric. Mass Median Aerodynamic Diameter is the aerodynamic diameter below which 50% of the particle population lies, on the basis of mass. It therefore defines the central tendency of the APSD, relative to the upper limit for successful delivery to the lung.
Determining MMAD from the preceding plot clearly calls for interpolation. With the cumulative plot, identifying the stage cut-off diameter corresponding to 50% requires sigmoid curve-fitting. Results are dependent on the chosen curve-fitting method though encouragingly, simple two-point interpolation has been shown to be relatively reliablei. More recent work by expert groups and the USP provide useful background information in this areaii,iii.
Interpolation with the log-probit plot calls for simpler, straight-line fitting with Probit 5 corresponding to a cumulate % of 50%.
Defining and determining GSD
GSD adds complementary insight to MMAD by quantifying the breadth or spread of the APSD. Geometric Standard Deviation is a measure of the difference between values in the distribution and the mean. In practical terms, smaller GSD values mean a narrower or tighter distribution around the MMAD.
However, GSDs are only relevant for populations that exhibit a log-normal distribution. Many OIPs do not, and it is hard to predict which will.
For OIPs that do not exhibit a log-normal distribution, alternative measures of spread can fulfil a similar purpose. Such measures include the 10th and 90th percentile stage cut-off diameters, and/or span.
Either way looking at the breadth of the APSD helps to focus attention on both the coarse and fine ends of the distribution. Both are potentially problematic with respect to drug delivery and as a result a low GSD, indicating a narrow APSD spread, tends to be the goal.
The unique relevance of FPF
In combination, MMAD and GSD are valuable metrics for comparing products or batches. That said, they provide no insight into the fraction of the dose in the size range of interest. Products with a closely similar MMAD and GSD could exhibit clinically significant differences in dose delivered to the lung. Including ISM or comparable metrics relating to delivered dose is therefore vital.
Fine Particle Dose (FPD) and FPF provide a good illustration of this point.
FPD is the sub-5 µm fraction of the dose that on the basis of aerodynamic size would be likely to deposit in the lung.
Expressing this dose as a fraction of the delivered dose, quantifies FPF, where:
FPF = FPD/Delivered Dose
Both FPF and FPD are highly relevant for evaluating device/delivery performance. FPF quantifies the success of dose dispersion to a respirable size, relative to dose emission/device emptying. FPD quantifies in absolute terms the likely success of drug delivery with different device/formulation options.
Currently values of MMAD, GSD and FPF/FPD dominate OIP reporting, with other, often product-specific stage groupings adding detail. However, our collective understanding of how best to analyse cascade impaction data continues to evolve.
Additional metrics, simpler analysis
EDA is the result of efforts to refine the processing of cascade impaction data in line with informational need. Principally, cascade impaction measurements answer relatively simple questions. In QC the goal is to determine whether batches are the same, and within specification. In R&D it may be sufficient to know only whether FPD is higher or lower.
This begs the question: Is there a simpler way to process cascade impaction data for routine use? Detailed analysis by leading experts suggests there is.
Using cascade impaction data to generate just two mass fractions provides sufficiently sensitive sample differentiation to meet many routine requirements. Large Particle Mass (LPM) is the mass of drug above a boundary particle size, Small Particle Mass (SPM) the mass below. The boundary is best set to maximise sensitivity and is product-specific, though it tends to lie close to the MMAD. Together, changes in LPM/SPM and ISM are sufficient to detect pertinent changes in APSD.
The sensitivity and simplicity of this approach make it especially appealing for QC. That said, certain types of R&D study are amenable to a strictly analogous approach.
We’ll be returning to EDA and its practical incarnation – Abbreviated Impactor Measurement – in a later blog. In the meantime, if you want to dig deeper into data analysis then webinar is a great place to start. Alternatively, check out our cascade impaction software if you’ve learned enough already!
i Stimuli to the Revision Process, “Generalized Simplified Approaches for Mass Median Aerodynamic Determination,” Pharmacopeial Forum 36 (3) (2010).
ii Stimuli to the Revision Process ‘Proposals for Data Interpretation in the Context of Determination of Aerodynamic Particle Size Distribution Profile for Orally Inhaled Products’ USP Pharm Forum 43(3) (2017).
iii USP <1604> Presentation of Aerodynamic Particle Size Distribution (APSD) Measurement Data for Orally Inhaled Products, Dec 2023.








