Dissolution tests is synonymous with oral solid dosage (OSD) products but transdermal drug delivery systems (TDDS) and orally inhaled and nasal drug products (OINDPs) can also benefit…
For orally administered drugs the first reports of a link between dissolution and rate of absorption in vivo date back to the 1950s. The subsequent proliferation of dissolution testing is attributable to the volume and diversity of today’s OSD industry. But progressive application away from the OSD mainstream is also a factor.
In this blog we’ll examine the application of dissolution testing for two complex pharmaceutical formats. For TDDS and OINDPs dissolution testing can help to build detailed product understanding, enhance performance, and safeguard product quality. Find out how.
An introduction to TDDS
For drug delivery via the skin there are two distinct classes of product: semisolids and TDDS, typically transdermal patches. Semisolids are creams, lotions, ointments, and gels and predominantly applied for topical relief. In contrast, transdermal patches focus on systemic drug delivery. Key applications include pain relief, hormone delivery, and drugs for neurological conditions such as attention deficit hyperactivity disorder and Alzheimer’s.
Transdermal patches enjoy a high degree of patient acceptance. Easily applied to the skin they can provide consistent dosing with no further attention, for periods of up to 7 to 9 days. Treatment is easy to stop, and there is no risk of damage to the drug from first pass metabolism in the gastrointestinal tract.
However, delivering drugs transdermally means penetrating the skin, a barrier expressly designed to prevent the ingress of potentially damaging molecules. Sustaining a consistent drug delivery rate for the lifetime of the product is a further challenge.
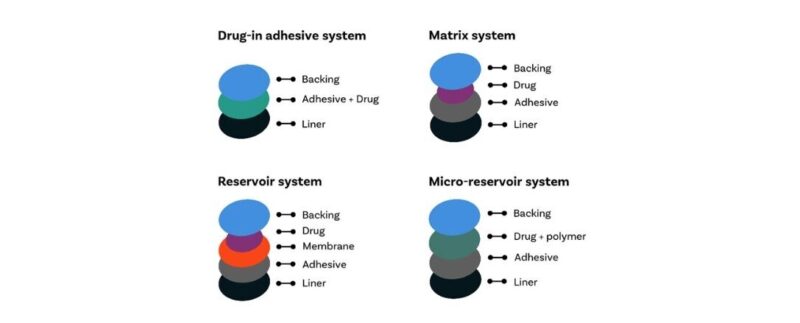
Figure 1: Types of transdermal patches
To achieve these goals transdermal patches are necessarily complex, multi-layered assemblies, incorporating backing, drug, adhesive and liner. Drugs are held in a membrane-contained reservoir, or in a polymer matrix, or in micro-reservoirs, a composite approach. Drug-in-adhesive systems are also an option.
The value of dissolution tests for TDDS
Dissolution tests quantify the rate of drug release from a given transdermal assembly under controlled conditions. Compendial test methods for assessing this aspect of TDDS performance are analogous to those for OSD products with the pharmacopoeias specifying use of Paddle over Disk; Rotating Cylinder; or Reciprocating Holder (Ph. Eur. only) apparatuses. Apparatus 2 (Paddle over Disk) is readily modified for TDDS testing and simple to use making it the preference for many. Enhancing methods to include assessment of the kinetics of membrane transfer, to assess the rate of drug penetration through the skin, maximises their utility.

In product development the resulting data directly support the manipulation of drug release rate, and lag time, to meet clinical goals. Lag time is associated with the need for drug accumulation at the skin surface to drive skin penetration. For some products a substantial drug concentration gradient is necessary, resulting in an appreciable, clinically significant lag time.
Using dissolution testing developers can work towards products that act sufficiently quickly and perform consistently for a defined period. Furthermore, since release rate and lag time are performance defining, such testing is valuable through to final quality control.
The challenge of OINDPs
The primary motivation for delivering drugs to the nose or lung is to achieve localised therapeutic effect. Every day, inhalers provide potentially life-saving protection and relief for patients suffering from conditions such as asthma and chronic obstructive pulmonary disease. Products for allergic rhinitis and hay fever dominate the nasal drug product marketplace. For respiratory care, OINDPs essentially offer an unbeatable combination of rapid, targeted action with minimal systemic exposure.
Delivering an appreciable fraction of the drug to the target deposition site is a defining challenge, notably for pulmonary delivery. As previously discussed, deposition in the lung calls for dose dispersion to a particle size of less than 5 µm. For intranasal the goal is a size distribution centred on a particle size of 30 – 120. Once particles reach the target deposition site dissolution and permeation into the surrounding tissues is an essential precursor to therapeutic effect. As a result, the dissolution behaviour of inhaled drugs has long been a topic of interest.
That said, motivation for the application of dissolution testing for OINDPs is now increasing. Recent updates to product specific guidances (PSGs) from the FDA include the use of inhaled dissolution as part of an alternative approach to establishing bioequivalence. More generally, efforts to use these routes for systemic delivery also intensify interest in dissolution behaviour. Optimising OINDPs for systemic drug delivery relies on improving our understanding of in vivo fate with dissolution a first step towards therapeutic efficacy.
The value of dissolution testing for OINDPs
For orally inhaled drugs, dissolution testing helps to identify drugs that may exhibit poor efficacy due to limited solubility. The fine particle size of these drugs, combined in many instances with high solubility, mitigate towards rapid dissolution. However, volumes of fluid in the lung are minimal, and of varying composition, depending on disease state and lung region. Conditions for dissolution are therefore neither consistent nor optimal. As we embrace pulmonary delivery for a broader range of drugs there is a growing risk that under these suboptimal conditions dissolution will be a rate limiting step.
The situation for intranasal drug delivery is somewhat similar. While many nasal drug products are solution-based sprays, the use of suspensions and nasal powders is reliant on timely dissolution. Mucociliary clearance mechanisms sweep contaminants from the nose extremely effectively. Sufficiently rapid dissolution is therefore essential, notably for systemic drugs, which are just beginning their in vivo journey.
For all OINDPs, dissolution testing may be key to identifying subtle, clinically relevant, differences between test and reference products.
These motivations for dissolution testing for OINDPs are well-understood and there are commercial solutions available for implementation. However, there are currently no compendial methods in place. Given the complex physiology of both the nose and lung it is a challenge to establish representative methods. Debate over the practicalities and relevance of alternative strategies therefore continues.
Looking ahead
Looking across OSD products, TDDS, and OINDPs we can see an arc of application of dissolution testing. Ultimately, all drugs must dissolve to exert an impact in vivo, and the relevance of dissolution behaviour is correspondingly broad. That said, shaping dissolution methods to address the issues associated with specific products is crucial to maximise utility.
For TDDS, it is the ability to enable drug molecules to penetrate the skin that limits the use of the route. Enhancing drug penetration by either mechanical or chemical means is the defining focus of research activities and has been for many years. Refining dissolution methods to encompass membrane transfer is therefore a logical progression. Such testing is already well-established with compendial methods in place.
For OINDPs, it is our ability to consistently deliver drug to a target deposition site, in the face of patient variability that continues to challenge. Beyond this, understanding in vivo fate is becoming increasingly important. Potentially beneficial tactics such as physiologically-based pharmacokinetic modelling (PBPK), which could accelerate and improve product development call for in-depth insight. A better understanding of dissolution behaviour at the deposition site would support such activities. Furthermore, dissolution testing is beginning to find application in the demonstration of bioequivalence and may ultimately become part of QC.
Going forward, it therefore seems likely that dissolution testing will establish for OINDPs in the same way as it already has for TDDS and indeed OSD. In the meantime, we debate the issues and continue to develop best practice. In future blogs we’ll be returning to these issues in greater detail. If you’d like to read more ahead then…